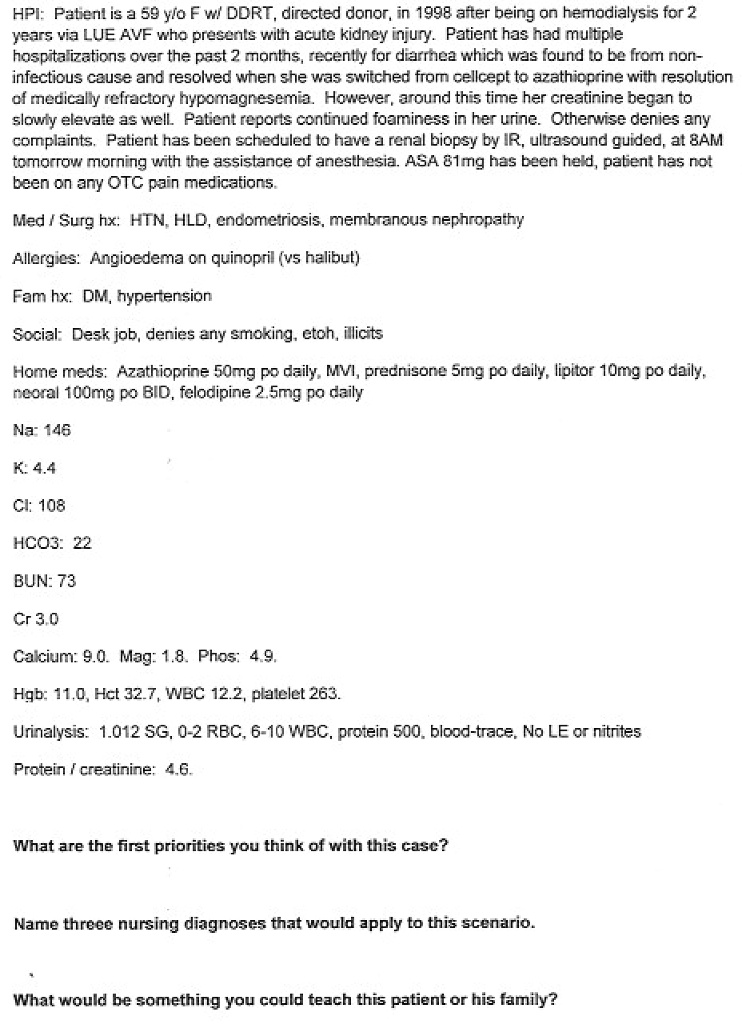
HPI Patient is a 59-year-old female with DDRT-directed donor in 1998 after being on hemodialysis for 2 years via LUE AVF who presents with acute kidney injury. The patient has had multiple hospitalizations over the past 2 months, recently for diarrhea which was found to be from a non-infectious cause and resolved when she was switched from Cellcept to azathioprine with resolution of medically refractory hypomagnesemia. However, around this time her creatinine began to slowly elevate as well. The patient reports continued foaminess in her urine. Otherwise, she denies any complaints. The patient has been scheduled to have a renal biopsy by IR, ultrasound-guided, at 8 AM tomorrow morning with the assistance of anesthesia. ASA 81mg has been held, and the patient has not been on any OTC pain medications.
Med/Surg hx: HTN, HLD, endometriosis, membranous nephropathy
Allergies: Angioedema on quinapril (vs halibut)
Fam hx: DM, hypertension
Social: Desk job, denies any smoking, alcohol, illicit drugs
Home meds: Azathioprine 50mg po daily, MVI, prednisone 5mg po daily, Lipitor 10mg po daily, Neoral 100mg po BID, felodipine 2.5mg po daily
Na: 146
K: 4.4
CI: 108
HCO3: 22
BUN: 73
Cl: 10
Calcium: 9.0, Mag: 1.8, Phos: 4.9
Hgb: 11.0, Hct: 32.7, WBC: 12.2, platelet: 263
Urinalysis: 1.012 SG, 0-2 RBC, 6-10 WBC, protein 500, blood-trace. No LE or nitrites
Protein/creatinine: 4.6