Please do not use or disclose the information contained here for any purposes other than ones permitted under HIPAA.
Back Print
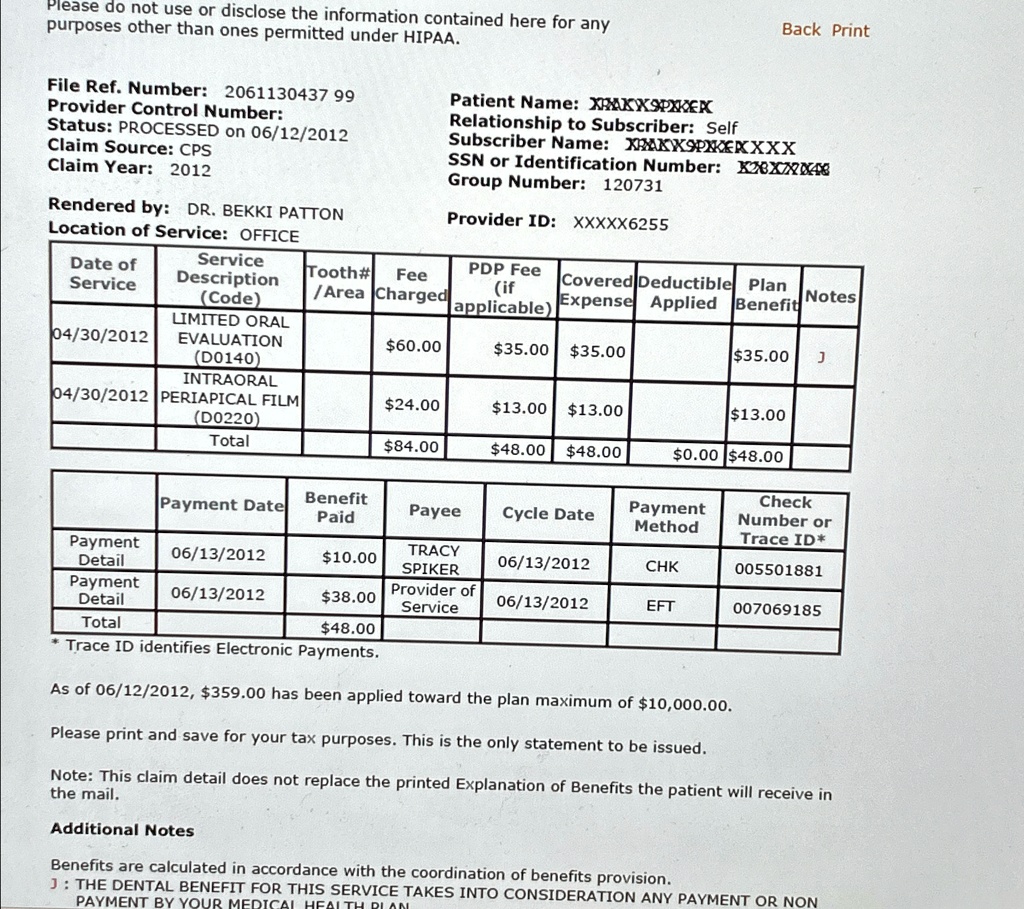
File Ref. Number: 206113043799
Provider Control Number:
Status: PROCESSED on 06/12/2012
Claim Source: CPS
Claim Year: 2012
Rendered by: DR. BEKKI PATTON
Location of Service: OFFICE
Patient Name: XFXUXSPXKER
Relationship to Subscriber: Self
Subscriber Name: XRXXSPNXXXXX
SSN or Identification Number: XXXXX2CE
Group Number: 120731
Provider ID: XXXXX6255
[table[[Date of],[Service]], [Service],[Description], [(Code)]], [Tooth#],[Area], [Fee],[Charged], [PDP Fee], [(if],[applicable)], [Covered],[Expense], [Deductible],[Applied], [Plan],[Benefit], Notes]
(04/30/2012, [LMITED ORAL],[EVALUATION], [(D0140)], $60.00, $35.00, $35.00, $35.00, $35.00, J
Please do not use or disclose the information contained here for any purposes other than ones permitted under HIPAA.
Back Print
File Ref. Number: 206113043799
Provider Control Number:
Status: PROCESSED on 06/12/2012
Claim Source: CPS
Claim Year: 2012
Patient Name: XKXPXKEK
Relationship to Subscriber: Self
Subscriber Name: XAKX9PXKXXXX
SSN or Identification Number: XX4
Group Number: 120731
Provider ID: XXXXX6255
Rendered by DR. BEKKI PATTON
Location of Service: OFFICE
Date of Service Tooth# Fee PDP Fee Service Description (if Covered Deductible /Area Plan (Code) Charged Expense Applied Notes applicable) Benefit
LIMITED ORAL 04/30/2012 EVALUATION $60.00 D0140 $35.00 $35.00 $35.00 J
INTRAORAL 04/30/2012 PERIAPICAL FILM $24.00 $13.00 D0220 $13.00 $13.00
Total $84.00 $48.00 $48.00 $0.00 $48.00
Payment Date Benefit Paid Payee Cycle Date Payment 06/13/2012 $10.00 TRACY Detail SPIKER 06/13/2012 Payment 06/13/2012 $38.00 Provider of Detail Service 06/13/2012 Total $48.00 Trace ID identifies Electronic Payments
Payment Method
Check Number or Trace ID* 005501881 CHK EFT 007069185
As of 06/12/2012, $359.00 has been applied toward the plan maximum of $10,000.00
Please print and save for your tax purposes. This is the only statement to be issued. the mail.
Note: This claim detail does not replace the printed Explanation of Benefits the patient will receive in Additional Notes
Benefits are calculated in accordance with the coordination of benefits provision.
J: THE DENTAL BENEFIT FOR THIS SERVICE TAKES INTO CONSIDERATION ANY PAYMENT OR NON PAYMENT BY YOUR MEDICAI